Burnout, you may have heard the term going round at the moment. For some the term is relatively new and for others it’s a phrase that’s being thrown around a lot. Many people are experiencing symptoms of burnout and don’t even realise what they are experiencing. It can also be mistakenly identified as anxiety and depression however burnout is all about your relationship between work and home.
Originally burnout was named by an American psychologist Herbert Freudenberger. It was used to describe the consequences of high stress jobs. However, burnout can effect anyone from students, homemakers, office workers, artists and so on. In 2019, WHO revised their definition of the Phenomenon. They describe burnout as a symptom of chronic stress from work that has not been mangaed.
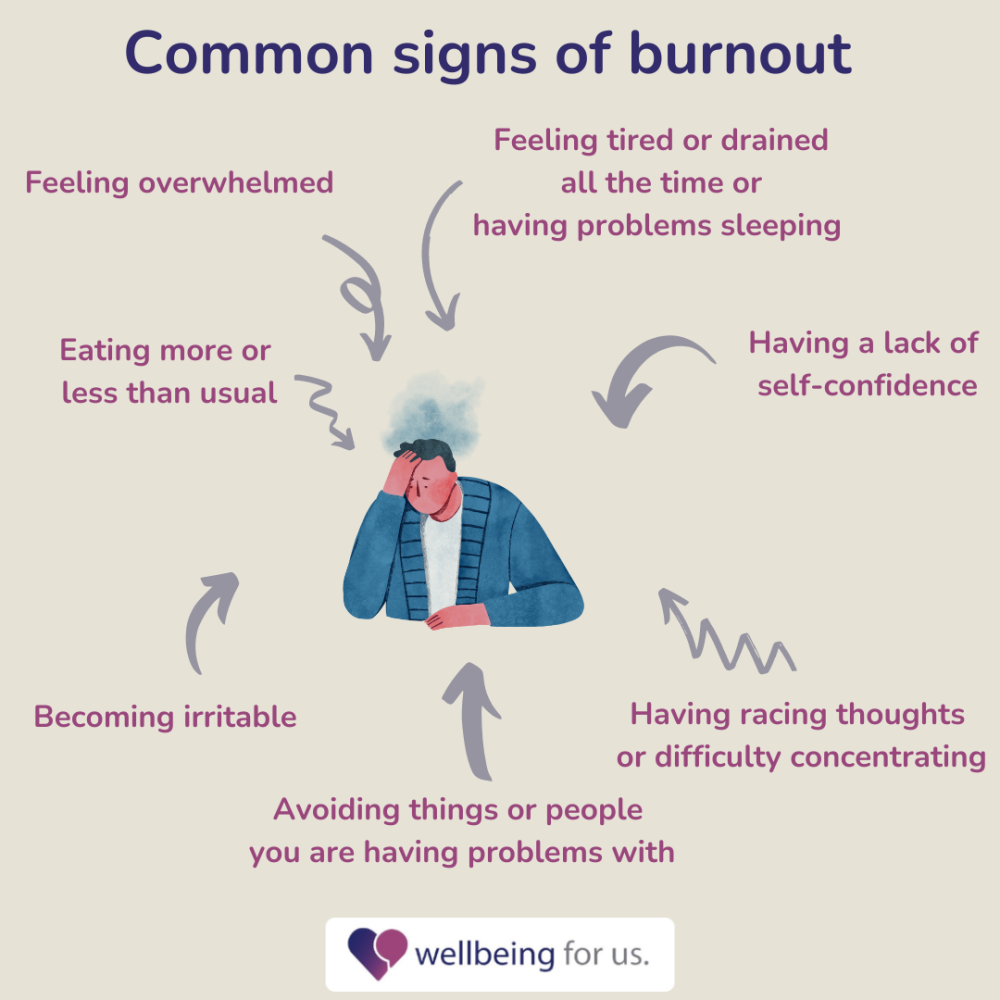
Common signs of burnout
Feeling tired or drained all the time or having problems sleeping
Feeling overwhelmed
Having a lack of self-confidence
eating more or less than usual
avoiding things or people you are having problems with
Having racing thoughts or difficulty concentrating
Becoming irritable
Burnout does not go away by its self however there are steps you can take to help. One big step that people forget is self care. Self care is super important as you can forget that you’re not a robot. You need time for you. It’s important to nourish yourself and set achievable goals.
A good start on the road to recovery is to identify what the main causes of stress are. Then figure out what you can do about it. This is to give your brain away to think about the solution. Another way to help is to leave work at work. Now this is easier said than done but the stress is what leads to the burnout. Start to prioritise a work-life balance so that you can recharge for the next day.
The road to recovery can take a while and it may not make a difference straight away however it will eventually start to help.
References
Burn out and how to avoid it Author: Liggy Webb
burnout prevention and treatment Authors: Melinda Smith, M.A., Jeanne Segal, Ph.D., and Lawrence Robinson
The official WHO website www.who.int/news/item/28-05-2019-burn-out-an-occupational-phenomenon-international-classification-of-diseases
Trichotillomania or ‘Trich’ involves obsessive compulsive hair pulling from any area of the body, most often from the scalp, eyebrows and eyelashes. It is often done to relieve tension as with OCD but can also be done for pleasure or subconsciously and is commonly comorbid with other obsessive behaviours such as nail biting and skin picking[1].
Diagnosis: International Classification of Diseases (ICD-10)
“A disorder characterized by noticeable hair-loss due to a recurrent failure to resist impulses to pull out hairs. The hair-pulling is usually preceded by mounting tension and is followed by a sense of relief or gratification. This diagnosis should not be made if there is a pre-existing inflammation of the skin, or if the hair-pulling is in response to a delusion or a hallucination.”[2]
The Lived Experience
Hair pulling often brings with it embarrassment and shame, heightening risk of social isolation, depression and anxiety[3]. The physical effects are also adverse, in terms of scarring and infections in areas that are pulled from. Furthermore, it is common for individuals with trichotillomania to eat their hair (trichophagia), which can lead to hair balls building up in the digestive tract, causing uncomfortable and potentially life-threatening digestive complications and obstructions[4]
Treatments for Trichotillomania
Cognitive Behavioural Therapy (CBT): CBT for trichotillomania comes in the form of habit reversal training, whereby the patient and therapist work to replace maladaptive habits and thoughts with more rational ones. For example, identifying and avoiding potential triggers for pulling or focusing the anxiety on something less harmful such as a stress ball.
Family therapy: Involving family in behavioural treatment plans can increase their effectiveness, particularly for children with trichotillomania[5]
Relaxation Training: Breathing techniques, yoga and meditation can help those with trichotillomania process feelings of tension and offer an alternative relief to hair pulling[6]
Medication: As with most obsessive-compulsive disorders, medication is not recommended as a direct treatment, however antidepressants can be used to treat commonly comorbid illnesses such as depression and anxiety[7]
References
Keuthen, N. J., Curley, E. E., Scharf, J. M., Woods, D. W., Lochner, C., Stein, D. J., … & Grant, J. E. (2016). Predictors of comorbid obsessive-compulsive disorder and skin-picking disorder in trichotillomania. Annals of Clinical Psychiatry: Official Journal of the American Academy of Clinical Psychiatrists, 28(4), 280-288.
Grant, J. E., Redden, S. A., Leppink, E. W., & Chamberlain, S. R. (2017). Trichotillomania and co-occurring anxiety. Comprehensive psychiatry, 72, 1-5.
Özten, E., Sayar, G. H., Eryılmaz, G., Kağan, G., Işık, S., & Karamustafalıoğlu, O. (2015). The relationship of psychological trauma with trichotillomania and skin picking. Neuropsychiatric disease and treatment, 11, 1203–1210. https://doi.org/10.2147/NDT.S79554
Grant, J. E., & Chamberlain, S. R. (2018). Salivary sex hormones in adolescent females with trichotillomania. Psychiatry research, 265, 221-223.
[1] Snorrason, I., Belleau, E. L., & Woods, D. W. (2012). How related are hair pulling disorder (trichotillomania) and skin picking disorder? A review of evidence for comorbidity, similarities and shared etiology. Clinical psychology review, 32(7), 618-629.
[2] World Health Organization. (2019). International statistical classification of diseases and related health problems (11th ed.). https://icd.who.int/
[3] Grant, J. E., & Chamberlain, S. R. (2016). Trichotillomania. American Journal of Psychiatry, 173(9), 868-874.
[4] Snorrason, I., Ricketts, E. J., Stein, A. T., & Björgvinsson, T. (2021). Trichophagia and trichobezoar in trichotillomania: a narrative mini-review with clinical recommendations. Journal of Obsessive-Compulsive and Related Disorders, 31, 100680.
[5] Flessner, C. A., Penzel, F., Board, T. L. C. S. A., & Keuthen, N. J. (2010). Current treatment practices for children and adults with trichotillomania: consensus among experts. Cognitive and Behavioral Practice, 17(3), 290-300.
[6] Sarah H, M., Hana F, Z., Hilary E, D., & Martin E, F. (2013). Habit reversal training in trichotillomania: guide for the clinician. Expert Review of Neurotherapeutics, 13(9), 1069-1077.
[7] Sani, G., Gualtieri, I., Paolini, M., Bonanni, L., Spinazzola, E., Maggiora, M., Pinzone, V., Brugnoli, R., Angeletti, G., Girardi, P., Rapinesi, C., & Kotzalidis, G. D. (2019). Drug Treatment of Trichotillomania (Hair-Pulling Disorder), Excoriation (Skin-picking) Disorder, and Nail-biting (Onychophagia). Current neuropharmacology, 17(8), 775–786. https://doi.org/10.2174/1570159X17666190320164223
Narcolepsy is a sleep disorder caused by neurological changes that leads to difficulties regulating ones sleep-wake cycle. It can be seen in sudden sleep ‘attacks’ that can’t be controlled and cataplexy, which is when the individual suddenly loses muscle tone.
Diagnosis
Narcolepsy is diagnosed in the Diagnostic and Statistical manual of mental disorders (APA 2013) according to the following criteria:
Recurrent periods of an irrepressible need to sleep, lapsing into sleep, or napping occurring within the same day. These must have been occurring at least 3 times per week over the past 3 months.
The presence of at least one of the following:
Episodes of cataplexy, occurring at least a few times per month, and as defined by either:
In individuals with long-standing disease, brief (sec to min) episodes of sudden, bilateral loss of muscle tone with maintained consciousness that are precipitated by laughter or joking
In children or in individuals within 6 months of onset, spontaneous grimaces or jaw-opening episodes with tongue thrusting or global hypotonia, without any obvious emotional triggers.
Hypocretin deficiency, as measured by cerebrospinal fluid (CSF) hypocretin-immunoreactivity values of one-third or less of those obtained in healthy subjects using the same assay, or 110 pg/mL or less.
Nocturnal sleep polysomnography (PSG) showing rapid eye movement (REM) sleep latency of 15 minutes or less, or a multiple sleep latency test (MSLT) showing a mean sleep latency of 8 minutes or less and more than 2 sleep onset rapid eye movement periods (SOREMPs).
Treatments
Narcolepsy can cause significant difficulties and dangers in everyday life and unfortunately there is no cure, but the are changes that can be made to help to alleviate symptoms. These include:
Lifestyle Changes:
Diet: Eat a balanced diet with whole foods and limited processed foods, eating regularly throughout the day and not immediately before bed. Avoid caffeine, nicotine and alcohol as these disturb sleep
Regular Exercise: This aids with forming healthy sleep patterns and general wellbeing
Take Naps: By scheduling naps, you can reduce the risk of sudden ‘sleep attacks’
Talk to others: Narcolepsy is a misunderstood illness and explaining it to those close to you helps form a base of support
Medication:
Stimulants such as modafinil can help individuals stay awake for longer during the day but may bring adverse side effects such as nausea and anxiety
Antidepressants such as selective serotonin reuptake inhibitors help to reduce narcolepsy episodes by reducing the amount of rapid eye movement sleep. Other antidepressants used include serotonin-noradrenaline reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs)
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: Author.
Anderson, T., Bandi, M., Bromley, K. D., Nino, M., & Terekhov, K. (2003). Narcolepsy.
M. Billiard, V. Pasquié-Magnetto, M. Heckman, B. Carlander, A. Besset, Z. Zachariev, J. F. Eliaou, A. Malafosse, Family Studies in Narcolepsy, Sleep, Volume 17, Issue suppl_8, December 1994, Pages S54–S59, https://doi.org/10.1093/sleep/17.suppl_8.S54
Mehta, R., Jiwanji, M., Singhal, R., Gillam, E., Lockwood, K., & Quarmley, M. (2021). The Social and Emotional Toll of Narcolepsy. Undergraduate Works.
What we eat doesn’t just affect our physical wellbeing but also impacts our mental health and overall mood. By taking this more holistic approach to wellbeing, we can lead healthier lifestyles and reduce the risk of physical and mental illness.
In general, a more ‘Mediterranean’ diet with whole foods, vegetables and fish is better for wellbeing compared to a more ‘Western’ diet of processed foods and red meats. However, food and wellbeing aren’t simply interrelated on the basis of what we eat but also when we eat. It is important to eat regularly as mood can dip when our blood sugar levels are low and eating regularly helps keep them at a stable level. It is important not to skip breakfast and eat smaller meals throughout the day and avoid foods that make your blood sugars rapidly increase, such as sugary soft drinks. Furthermore, it is key to stay hydrated as dehydration can reduce our memory ability and focus and water is also key in serotonin production which helps improve mood[1]
Understanding Eating Disorders:
While food is a source of pleasure for some, it can unfortunately be a source of anxiety and eating disorders can quite suddenly develop and become very harmful to our physical and mental wellbeing, Eating disorders such as anorexia and bulimia nervosa require professional intervention from a therapist and/or medication. Information on bulimia nervosa diagnosis and treatments can be seen in this article: https://www.linkedin.com/pulse/bulimia-nervosa-diagnosis-impacts-causes-treatments-/
References
Ocean, N., Howley, P., & Ensor, J. (2019). Lettuce be happy: A longitudinal UK study on the relationship between fruit and vegetable consumption and well-being. Social Science & Medicine, 222, 335-345.
Grosso, G., Galvano, F., Marventano, S., Malaguarnera, M., Bucolo, C., Drago, F., & Caraci, F. (2014). Omega-3 fatty acids and depression: scientific evidence and biological mechanisms. Oxidative medicine and cellular longevity, 2014.
Huntley, E. D., & Juliano, L. M. (2012). Caffeine Expectancy Questionnaire (CaffEQ): construction, psychometric properties, and associations with caffeine use, caffeine dependence, and other related variables. Psychological assessment, 24(3), 592.
Golomb, B. A., & Bui, A. K. (2015). A fat to forget: Trans fat consumption and memory. Plos one, 10(6), e0128129.
Golomb, B. A., Evans, M. A., White, H. L., & Dimsdale, J. E. (2012). Trans fat consumption and aggression. PLoS One, 7(3), e32175.
Gangwisch, J. E., Hale, L., Garcia, L., Malaspina, D., Opler, M. G., Payne, M. E., … & Lane, D. (2015). High glycemic index diet as a risk factor for depression: analyses from the Women’s Health Initiative. The American journal of clinical nutrition, 102(2), 454-463.
[1] Popova, N.K., Ivanova, L. N., Amstislavskaya, T. G., Melidi, N. N., Naumenko, K. S., Maslova, L. N., & Bulygina, V. V. (2001). Brain serotonin metabolism during water deprivation and hydration in rats. Neuroscience and Behavioral Physiology, 31(3), 327-332.
Body Dysmorphic Disorder (BDD) is an increasingly common anxiety disorder characterised by obsessive concerns with body image and perception which is prevalent more so in children and youth.
Causes and Risk Factors:
Abuse or Neglect: Mistreatment, particularly during childhood either by a parent or at school increases the risk of developing obsessive compulsive disorders such as BDD[1]
Family and Genetics: Those with a family member with BDD are at higher risk of developing the disorder too, mainly due to learnt behaviours. Some genetic traits can increase risk too, including those that overlap with OCD[2]
Other Mental Disorders: Having other mental disorders such as anxiety or OCD increase vulnerability to developing BDD[3]
Fear of Isolation: Someone may be made to feel that they need to shape their appearance to be accepted by a certain group such as models or bodybuilders, which can increase the risk of BDD
Perfectionism: Individuals who have neurotic personalities are likely to become obsessive about their appearance, often exacerbated by the constant presentation of ‘perfect’ male and female bodies in the media[4]
Treatments:
Cognitive Behavioural Therapy (CBT): CBT helps the patient recognise and understand their triggers for insecurities and anxiety surrounding body image. It helps them recognise that these beliefs are irrational and harmful and form a more realistic and positive view of their appearance.
Exposure and Response Prevention: This is a common aspect of CBT when treating BDD, involving gradual exposure to a stimulus that can trigger body related anxiety such as being in crowded places. The ‘response prevention’ aspect involves working with the patient to reduce compulsive behaviours, such as constant mirror checking.
Medication: Selective Serotonin Reuptake Inhibitors (SSRIs), typically used to treat depression can be effective in reducing BDD symptoms through regulating neurotransmitter levels[5]
[1] Himanshu, A. K., Kaur, A., & Singla, G. (2020). Rising dysmorphia among adolescents: A cause for concern. Journal of family medicine and primary care, 9(2), 567.
[2] Monzani, B., Rijsdijk, F., Iervolino, A. C., Anson, M., Cherkas, L., & Mataix-Cols, D. (2012). Evidence for a genetic overlap between body dysmorphic concerns and obsessive-compulsive symptoms in an adult female community twin sample. American journal of medical genetics. Part B, Neuropsychiatric genetics : the official publication of the International Society of Psychiatric Genetics, 159B(4), 376–382. https://doi.org/10.1002/ajmg.b.32040
[3] Chandler, C. G., Grieve, F. G., Derryberry, W. P., & Pegg, P. O. (2009). Are anxiety and obsessive-compulsive symptoms related to muscle dysmorphia. International Journal of Men’s Health, 8(2), 143-154.
[4] Himanshu, A. K., Kaur, A., & Singla, G. (2020). Rising dysmorphia among adolescents: A cause for concern. Journal of family medicine and primary care, 9(2), 567.
[5] Vashi, N. A. (2016). Obsession with perfection: Body dysmorphia. Clinics in Dermatology, 34(6), 788-791.
“Challenges are gifts that force us to search for a new centre of gravity. Don’t fight them. Just find a new way to stand.”
Oprah Winfrey
A woman’s position in society is forever changing. With everything that has happened this month every woman across the UK is questioning safety, boundaries, relationships and gender identity. There will always be change and society is constantly evolving.
What is important now is to show kindness and respect to one another, whilst listening to the voice of all women and then focussing on how to share personal stories and let voices be heard. That is what will bring about true change not through violence but through compassion and listening.
In its simplest form, resilience can be defined as “the process of adapting well in the face of adversity, trauma, tragedy, threats or even significant sources of stress”. In essence, resilience is our ability to ‘bounce back’ when faced with challenges.
Why is resilience important for mental health?
Resilience is key to help us overcome adversity and maintain good mental health in the face of challenges that we will all face in our lifetime, such as bereavement or unemployment. Adversity can be extreme, for example the war in Ukraine and the chronic stress, anxiety and forced migration this is causing civilians. Adversity increases risk of developing a mental illness; however, research has found incidence of mental illness to be reduced in those who are resilient.
Why are some people more resilient than others?
While many individuals are mentally resistant to the repercussions of traumatic events, many people will develop chronic, debilitating mental disorders that reduce their quality of life and daily functioning. Why some people are more resilient than others is a complex question with several factors to consider, including:
Political/Social landscape: Social and political systems differ in terms of their capability to support and promote the psychological wellbeing of groups and individuals. For example, the current resilience of Ukrainian armed forces and civilians is in part being supported by a strong government and international aid. This moral togetherness and material support facilitates individuals’ ability to cope and maintain mental resilience.
The importance of childhood: Research shows that being presented with and overcoming challenges in childhood without parental intervention helps build resilience through development of problem solving skills, emotion regulation and self-efficacy[3]. These experiences, ideally paired with a secure attachment to the parent are key to develop resilience skills which are carried into adulthood .
Social Connections: Research shows that more social connections, and close friendship groups help combat stress and anxiety, and aid in resilience against adversity, as evidenced during the Covid – 19 pandemic
Christmas is always a joyful time of the year. Families enjoy decorating the whole house together, decorating the Christmas tree, exchanging gifts , baking and decorating Christmas cookies and also making Christmas cards. It’s a wonderful season that brings loved ones together and connected in a special way.
However, with the cost of living rising the festive season is looking rather expensive for families this year. Usually hundreds of pounds are spent on Christmas gifts and presents for our loved ones.
The cost of living crisis has had a huge impact on the lives of people within the economy. Families have had to resort to local food banks to help feed themselves and their families this season. Some people may be worries about how to pay their bills and have an enjoyable Christmas. This can have a negative impact on mental health and put people in real mental crisis. It is hard to get into the spirit of the season. Thats why more than ever it is important to be kind to one another.
With all this going on it seems nearly impossible to stay positive and have an enjoyable Christmas. However there is always a solution to every problem.
Reach out to a loved one or neighbour. Is there someone you see in your area that could do with some food and a smile? Christmas is meant to bring families together even distant ones. Reach out to friends or families and don’t be alone with your feelings and worries. Or do something in your community go to help at a local crisis centre or food bank. Please access organisations or support groups that are available 24/7 and are always willing to help. It may be a difficult time but you are never alone.
Remember to not overwork yourself this period. The bills are coming in and the kids need to be happy but this can lead to negative issues that cause harm to your body and I doubt your family would choose money over your wellbeing. Finally, spend time with your family or community. It’s Christmas after all .
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. Cookies help us to analyse site usage and may be used to assist in our marketing efforts. By clicking “Accept”, you consent to the use of cookies on this site.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.






")


